Help for SwayStar™ (4.7.3.265)
The retrieve option recalls all
data that has been stored during previous sessions. It is accessed in two ways:
either Main Menu/Data/Retrieve and left click or simply click on the retrieve
icon ![]() .
All of the patient records are displayed in the upper box. The last name to
have appeared in the Retrieve Window is displayed when you first open the
program, have retrieved records in the database, or have set up a new patient.
Using the scroll bar to the right it is possible to display all patient names.
Whenever a patient name is selected (highlighted), the associated files appear
in the lower two boxes. To enable quicker searching, choose either the ID
number or the Name to arrange the listing order, and then type the appropriate
information in the white Search Filter field depending on whether the
search should be, by the ID number or by all or only the first part of a last
or first name or date of birth or a combination of all these.
.
All of the patient records are displayed in the upper box. The last name to
have appeared in the Retrieve Window is displayed when you first open the
program, have retrieved records in the database, or have set up a new patient.
Using the scroll bar to the right it is possible to display all patient names.
Whenever a patient name is selected (highlighted), the associated files appear
in the lower two boxes. To enable quicker searching, choose either the ID
number or the Name to arrange the listing order, and then type the appropriate
information in the white Search Filter field depending on whether the
search should be, by the ID number or by all or only the first part of a last
or first name or date of birth or a combination of all these.
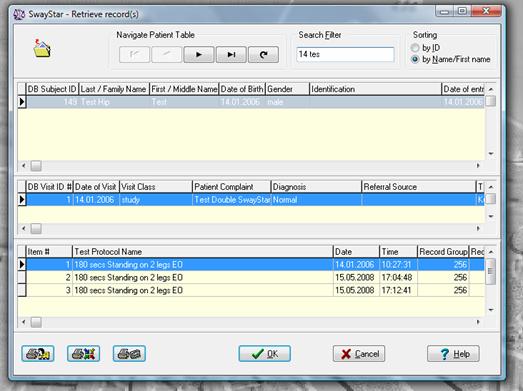
The headings for each box relate to the Manage Data windows described in section 5.1.3: Manage data.
Several retrieve options are available. You may select either to retrieve ALL records contained in a particular visit (second box) or individual protocols for the selected patient (third box) relative to a particular visit. Double left-click on the desired visit or protocol and the record(s) will immediately be displayed in the Data Analysis Screen. It is not necessary to retrieve individual records if you are interested in reviewing an entire session.
The last name that was selected and displayed as the name under which a recording was last saved will always be the name displayed when you first select the retrieve option. This is true whether you have just started the program, retrieved earlier records in the database or have setup a new patient.
The save function is available in five (5) instances: after entering details for the first time (new patient), after editing and details for an existing patient (edit options), after altering a time analysis window that recalculates the data for display, after markers are placed on the time histories or in the process of adding new recordings.
New patient details
New patient details will be saved to the database by clicking on OK (see description under Easy Start).
Editing
To change any details of an existing entry, it is necessary to edit them. The edit option is available via Manage. You may select edit by clicking on the button (right panel of the screen) or by using a common icon (see 5.1.3, below). When the edit option is active, you may either type in new details or select from a list. Accept or reject the new details by clicking the appropriate symbol:
|
|
|
|
Accept |
Reject |
After pressing the Accept button, the revised information is saved to the database.
The data will always remain as originally collected once a recording is been saved. However, it is possible to analyze and then save any part of the recording at a later time. Changing the analysis window does this.
Note: if the scaling values are altered in the Data Analysis Screen (see examples in 4.5.3 and 4.5.4), the new presentation of the data on the screen will not be saved. Such changes are for viewing purposes only.
Add Markers
If markers are added to the time plots, the position of these markers must be saved for later retrieval and before this information can be stored in the log file.
Adding new recordings
When you attempt to store new data into a currently selected visit record, the name of the subject will appear in red
![]()
It changes to black once you store the new recording. You will be reminded that the visit that is currently selected contains records older than 24 hours.
When you attempt to store data under a red name, the information relating to the name will be displayed. You have a number of options.
· If you are certain that you want to store data to this subject you can click OK.
· If the visit is older than 24 hours, you will be asked if this is really what you want to do. If your answer is NO, no action is taken and the recording is lost.
· If you answer YES, then the recording is stored under the old visit.
· If you did not want to use this patient name, you can hit the button next to the name information with .... on it and select another patient, or you can click the button labelled : to add another patient, which allows you to create a new visit or select an old visit by clicking the buttons next to the visit information. Then click OK and the data is stored under the selected name and visit.
It is best is to set up the patient and visit information ahead of time, then it will be in black and will automatically store in the correct place. Even if the name appears in black, it is still possible to change details when the name information is displayed.
Managing patient data accesses general information in the database. It is possible to add, edit and delete details that are not directly related to data analysis.
Navigate between the three options using the tabs.
![]()
There are a series navigation icons available in all data management windows. A drop-down Hint describes each.
|
|
|
|
|
|
|
|
|
Show first entry |
Show previous entry |
Show next entry |
Show last entry |
Add new entry |
Edit current entry |
Refresh screen |
Other common icons are:
|
|
|
|
|
|
|
|
|
Print Commands |
Accept |
Exit |
|
|||
|
Names of all patients |
All names and their complete records |
Current name plus a list off all recordings |
changes |
without saving |
|
|
The current data that has been selected in the three categories (patient, visit and record) are shown at the bottom of each window under Manage.
![]()
Patient
Patient information contains relevant details to enter (name, age, sex, etc.) and details that are automatically stored by the SwayStar™ program (subject number within the database, date of first visit, date on which details were modified and number of visits).
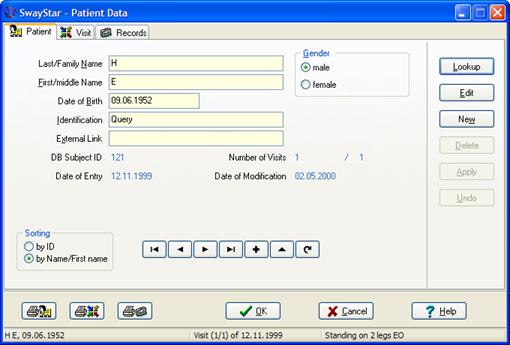
The meaning of the abbreviations and headings shown in the Patient window (in addition to name, sex and date of birth) are as follows:
|
Identification: |
Description of subject or other text |
|
External link: |
A number from an external database that a user can define; for instance, an identification number for a patient from the external database. |
|
DB Subject ID: |
Database subject identification number (automatically entered). Entries are numbered chronologically; i.e., the first patient entered into the database will always be DB Subject ID 1. |
|
Number of Visits: |
Number of visits entered in the Visit window |
|
Date of entry: |
Date subject was first entered into the database |
|
Date of modification: |
Date on which the most recent record was modified. |
Logged .csv files contain the following Patient information:
Identification, External link (useful for sorting purposes), Last Name, First Name, Gender with suffix as indicator of loss of balance for recording, Age not Date of Birth and DB Subject ID.
It is possible to use the navigation buttons to display database entries according to name or according to the identification relative to the order in which the subject was added to the database; e.g. the DB number. This option is available in the Sorting box where you select to sort by ID or by Name/ First name
Select either ID or Name 
The right-hand panel shows a set of buttons:
|
|
Lookup allows you to search for a subject from this screen without going to retrieve. |
|
|
Edit allows entry details to be changed (for instance, change the spelling of a name or enter an identification number). It is the same as :. |
|
|
New sets the details to a new default patient and allows completely new information to be entered. It is the same as ^. |
|
|
Delete is only available when there are no visits and records (or all deleted) for a particular patient. It is not possible to accidentally delete patient details if there are associated data. |
|
|
Apply is only available once Edit or New has been selected. Click to accept new entry data. It is the same as [. |
|
|
Undo is only available after Edit has been selected. It is the same as r and cancels changes that have not been saved.
|
Visit
A visit usually refers to a particular recording session although a visit can be added without completing a protocol or sequence.
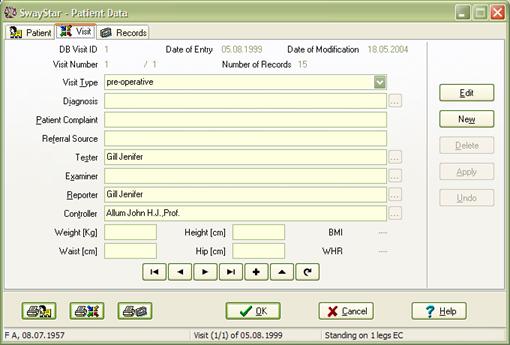
The user defines a list of optional
entries for several fields (diagnosis, examiner, tester, reporter and
controller). It is only possible to change the lists after Edit has been
selected (either with the edit button or by clicking on the ![]() icon). The list for visit type is
accessed by clicking on the
icon). The list for visit type is
accessed by clicking on the ![]() icon. This list cannot be changed.
icon. This list cannot be changed.
Clicking on New clears all windows
and also allows access to the lists. The rows for these entries are indicated
by ![]() .
Once edit or new has been selected, the greyed button becomes active and a new
window with one of these lists is opened. Using the standard icon commands (top
left corner of the screen), the list can be modified. To enter a choice, double
click on the appropriate row or click on OK.
.
Once edit or new has been selected, the greyed button becomes active and a new
window with one of these lists is opened. Using the standard icon commands (top
left corner of the screen), the list can be modified. To enter a choice, double
click on the appropriate row or click on OK.
There are two additional text fields the user can define: Patient Complaint and Referral source.
Logged.csv files contain the Patient Complaint and DB Visit ID.
The right-hand panel shows a set of buttons:
|
Edit to modify entry. |
|
|
Choose New to add a visit |
|
|
Delete a visit only if there are no records or if the delete visit option has been chosen in setting (see section 5.1.1). |
|
|
Accept data entry |
|
|
Clear new details if they have not been saved. |
|
If you wish to delete a name, you must first delete the visits under the name and all recordings under a visit or delete the visit altogether and its records providing the option has been selected under Options/Settings.
Record
A record is any saved protocol that has been completed for a particular patient.
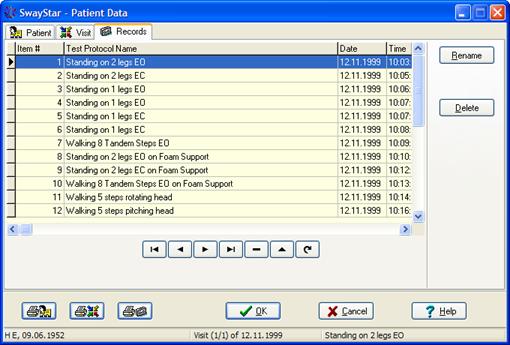
The abbreviations and heading shown in the Record window (and contained in logged .csv files) are as follows: The record screen shows relevant details of protocols for each visit. An explanation of the abbreviations and heading are as follows:
|
Item#: |
the protocol in the order entered for examination and in which the tests were performed |
|
Test Protocol Name: |
either a selected item or a user-defined item |
|
Date: |
date of test |
|
Time: |
time at which protocol data were collected |
(Note: The following columns and headings are not in the csv file; however, the log time is entered in the csv file.
|
Record Group: |
defines in code the setup type |
|
Record Type: |
defines in code the type of record (recording or report)
|
|
Date of modification: |
date of test |
|
Time: |
date on which the most recent record was |

The record name may be edited or the record may be deleted.
Renaming a record, changes the name only for the current subject and not for the protocol, in general. You may rename the protocol to any other relevant description, i.e., Standing on 2 legs EC assisted with two helpers (in this example).
Note: it is possible to rename user-defined protocols. Default factory protocols cannot be renamed or deleted.