Help for SwayStar™ (4.7.3.265)
Age at test: 61
Key Signs:
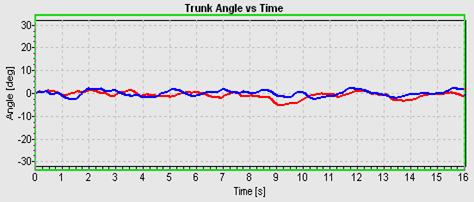
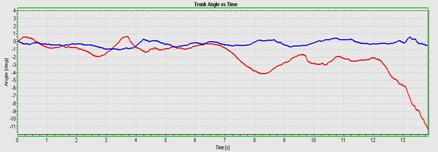
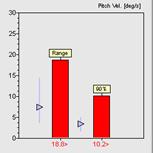
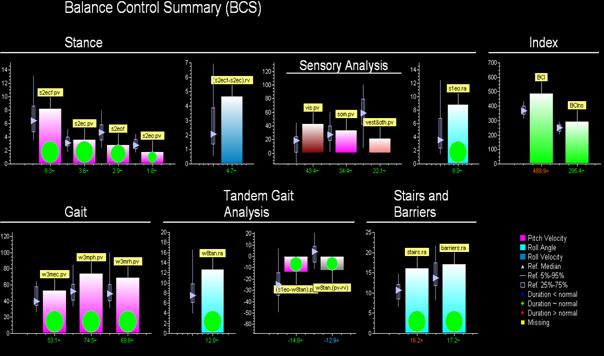
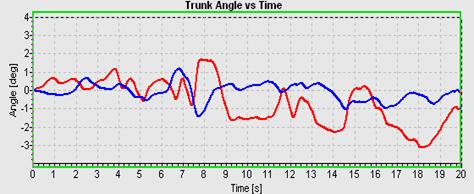
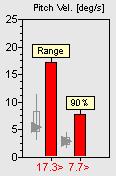
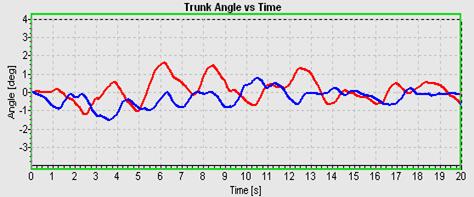
Shows the features typical of patients with balance problems due to vestibular loss - excessive trunk pitch velocity when tested standing on two legs, eyes closed, on foam. The patient tends to fall backwards and finally has to be caught at 13 seconds, see traces below.
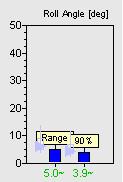
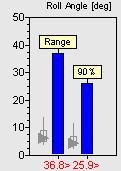
Standing on two legs, eyes closed, on foam. Red is pitch angle and blue is the roll angle. Peak-to-peak (range) and the 90% range for velocity is shown compared to normal values (median, 5% and 95% range are shown by the triangle and vertical bar).
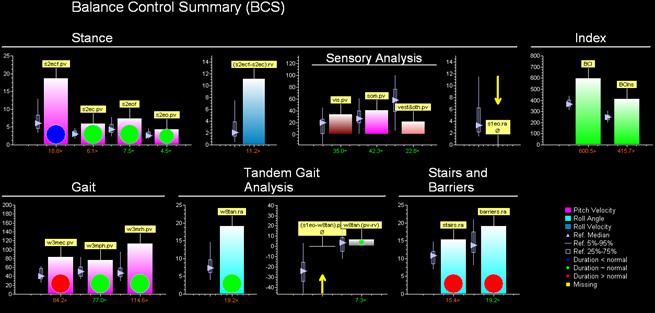
Summary Data:
Shows that for this patient, there are two general situations where poor balance control is most apparent. Tasks requiring exact control of trunk roll or tasks conducted with eyes closed. Thus the patient cannot perform 1-legged stance eyes open, has difficulties controlling trunk roll walking up stairs, and therefore performs this and other tasks (e.g. barriers) slowly. The patient also has excessive trunk sway walking eyes closed. Functionally this will mean that the patient will have difficulty with gait tasks requiring simultaneous fixation or in poor lighting conditions.
Indexes:
Show clearly that the patient has a balance problem.
Age at test: 62
Key Signs:
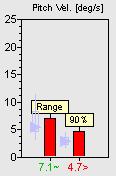
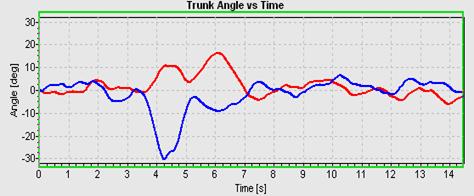
When the patient illustrated above is retested 3 months after the onset of the deficit, the question will be if there improvement is sufficient to permit the patient to work normally and if not the focus of continued rehabilitation. A clear improvement for the task of standing eyes closed on foam (see traces below) with reduction of pitch velocity to within the normal range (see columns at end of traces). Remaining deficit is excessive trunk roll when standing on 1 leg and when walking up and down stairs. Also trunk pitch while walking with head movements (pitching of head) has a value on the borderline of normal.
Standing on two legs, eyes closed, on foam.

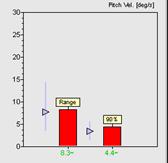
Summary Data:
Shows that stance control has improved considerably compared to the acute situation, however walking up stairs is still abnormal. The sensory analysis indicates the increased use of visual inputs to control trunk sway. The summary also suggests rehabilitation should concentrate on improving balance control during gait tasks with head movements or walking over obstacles, especially if this aspect is crucial during work performance.
Index:
Indicates an improvement in balance control compared to the acute status 3 months earlier.
Age at test: 55
Key Signs:
When the patient was retested 3 months after the onset of the deficit, there was 100% canal paresis in the caloric examination and a 40% remaining asymmetry in the horizontal VOR tests, even though an accompanying facial paresis had completely recovered. Examinations with SwayStar showed continuing instability in a number of tests at this time point: standing eyes closed on foam (see below), walking 3 metres with head pitching, walking 8 tandem steps (see traces below). The BCI was clearly pathological and sensory analysis showed no use of vestibular inputs. The question arose if improved balance control could be obtained with BII’s BalanceFreedom system as the focus of treatment. The clear improvement for the task of standing eyes closed on foam (see traces below) with reduction of pitch velocity to within the normal range (see columns at end of traces). An even greater improvement was obtained with the task of walking 8 tandem steps.
Standing on two legs, eyes closed, on foam.
Standing on two legs, eyes closed, on foam using BalanceFreedom biofeedback.
Walking 8 tandem steps.
Walking 8 tandem steps using BalanceFreedom biofeedback.